DRA is not limited to postpartum women; it is a condition also seen in men, athletes of both genders and children. For the purpose of this blog post we will concentrate on pregnancy since it is the most common preceding event for this condition,
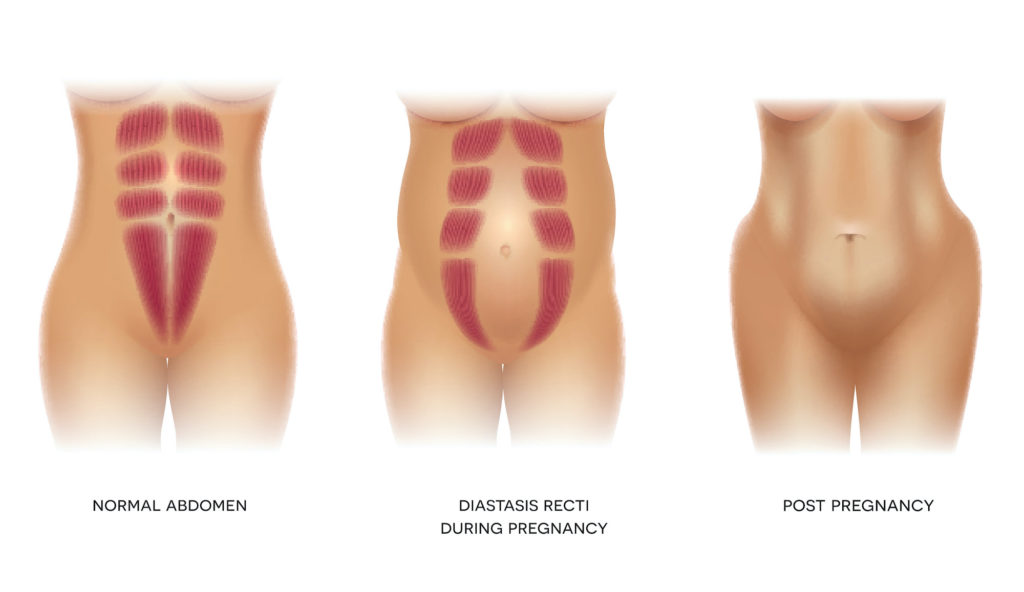
Diastasis recti, also known as DRA, happens when the midline of the abdominals starts to stretch, causing a separation where your abdominal muscles should meet. This is normal and occurs in 100% of pregnancies in order to make room for the growth of baby. It will also extend into the early post-natal recovery period during which your body is slowly returning to it’s pre-pregnant self.
The increasing weight during pregnancy combined with hormonal changes and altered posture are some of the main factors that increase the load on the abdominal wall and result in stretching of the linea alba. The linea alba is the connective tissue that connects the “6 pack” muscle into the midline of the abdomen. Once the linea alba has stretched, it can cause a bulging/doming appearance of the tummy and less commonly a sagging of the midline might be visible.
Now that we established that a DRA is a normal and expected outcome during pregnancy, the real question is “Has it come back to a normal state postpartum?”.
According to research, the distance between the two halves of your six-pack muscle is not likely to change much after 8 weeks postpartum unless you do something about it!
I recommend giving your body the initial 6-8 weeks post-partum to heal itself gently. During this time you are starting to care for your new born baby, feeding, carrying and all of this on reduced sleep. At the same time, your body is also slowly returning to it’s pre-baby self. Be kind to yourself, slowly and progressively reimplement physical activity. You may consider seeking the advice your local women’s health physiotherapist for a post-partum screening before returning to your favorite activity.
Having a persistent diastasis recti can disrupt the transfer of loads/pressure through the abdominal canister and in time can lead to issues such as low back pain, incontinence or prolapse.
Do we worry about the gap?
It is not just about the width of the linea alba but the depth of the separation and how it functions under load and during functional movements that we need to address.
Although a DRA wider than 2 fingers can be considered abnormal and may require attention, it really depends on what happens in the gap with respect to doming or sagging as previously mentioned.
For example, If you have a 3-4 finger separation yet your deep core layer activates with proper patterns and timing, you may not even show bulging and this is considered a functional DRA.
Conversely, you could have a 2 finger DRA with poor patterning and timing of core activation which may lead to significant doming/bulging and poor transfer of load through the core.

How will I know if I have abdominal separation?
- Belly bulge/doming or sagging appearance of the tummy
- Low back or pelvic pain
- Pelvic floor weakness ie. incontinence
- Feeling of “core” weakness
What can I do to fix it?
- Strengthen your pelvic floor and core and ensure proper patterning – you may want to talk to your therapist about how to optimally achieve this.
- Practice good posture. You should be upright and tall, with a small curve in your lower back. Your ribs should sit on top of your pelvis. Make sure you don’t have an excessive sway in the lower back and try not to push your hips forward. Leaning back too much can increase the load on your abdominal separation!

What should I avoid?
- Sitting up from a laying position (ie. when getting out of bed, try rolling to the side and then pushing up as a safer alternative)
- Constipation and straining on the toilet
- Heavy lifting
- Any movements where you can identify a bulge on your tummy could indicate poor load transfer and warrant modifying how you are doing the task. Your physiotherapist can help with that.
If you think you might have abdominal separation, book in to see your local women’s health physiotherapist for a thorough assessment and management to ensure you prevent worsening during pregnancy and make a full recovery after birth.
FAQ’s
Can you prevent abdominal separation?
You can’t prevent it! As mentioned above, all pregnant women will have some degree of abdominal separation by the end of their pregnancy. Although current research has not clarified the risk factors (see bellow) for a persisting DRA post-partum, you can minimize undue strain to the linea alba as it stretches by avoiding the following: constipation, heavy lifting, poor posture and heavy abdominal exercises that show signs of poor load transfer.
The risk factors for developing a DRA during pregnancy that does not resolve postpartum remain unclear. There is no statistical differences in women with persistent DRA at 6 months postpartum from those without when a recent research compared the following variables:
- Pre-Pregnancy BMI
- 6 month post-partum BMI,
- Weight gain during pregnancy,
- Baby’s birth weight,
- Abdominal circumference during pregnancy
- general hypermobility
Should you bother working on your separation during pregnancy or just wait until after birth?
There is allot you can do during pregnancy to optimise core strength, patterning and function. This will help you feel better in your later pregnancy, assist in your delivery and optimize your recovery afterwards. Even better yet, if you’re just finding out now you have a DRA and are on a subsequent pregnancy – IT’S NEVER TOO LATE. In fact it is a perfect opportunity to work on your DRA. Without getting to deep into the physiological details of why that is, what you need to know is that progressively loading the linea alba to help the collagen synthesis/reorganization (more on this bellow) is the way to recovery. What better way to progressively load the linea alba than a slowly growing belly?!
Do belly binding garments help?
Abdominal binding has been advocated for DRA but the binder should be applied properly and used with good judgement. Just to add some physiological mumbo jumbo – collagen syntheses and reorganization is required for repair of DRA at the linea alba, and for that reason loading the tissue is necessary. If the abdominal binder unloads the linea alba, then collagen synthesis/reorganization may take longer. When used in conjunction with proper movement training, abdominal binding can enhance recovery for some women in that the binder may provide sensory input and thereby facilitate the training. If however, the person wearing the binder merely “hangs out” in the binder, then minimal training will occur. With that said, binders should not be a stand-alone product in a women’s journey to DRA recovery.
Will the gap ever completely close?
Nope. Even in an individual who has never been pregnant, you would expect a slight separation as the two halves of the six pack muscle come into the midline at the linea alba. What is considered “normal” is a gap that is less than 2 fingers wide, which doesn’t bulge or sag and allows you to function well without pain or discomfort. In short, the aim should not be to eliminate the gap but instead to have a less than 2 finger gap with proper tensioning, good function and no bulge or sag.
What are the best exercises to do to repair a DRM?
There will be another blog post on this soon!